Reference Dr. Sally Shaywitz, Author of ‘ Overcoming Dyslexia’
Developmental dyslexia is an unexpected difficulty in reading. Unexpected refers to children and adults who appear to have all the factors necessary to become good readers: intelligence, motivation, and exposure to reasonable reading instruction – and yet struggle to read. Here, for ease of communication. We will refer to “developmental dyslexia” as simply “dyslexia”; it is also referred to as specific reading disability.
Dyslexia, first described over a century ago by a British physician, is the most common and most carefully studied of the learning disabilities, affecting 80% of all individuals identified as learning disabled.
The Basic Facts About Dyslexia
Who and how many are affected?
Similar to hypertension and obesity, dyslexia occurs in gradations. In other words, within the population, reading ability and reading disability occur along a continuum with dyslexia occurring in varying degrees of severity. Dyslexia is perhaps the most common neurobehavioral disorder affecting children, with prevalence rates ranging from 5-20%. Support for the high prevalence of dyslexia comes from the 2005 National Assessment of Educational Progress (NAEP) data which indicate that only 31% of fourth graders are performing at or above proficient reading levels. Sometimes, lower prevalence rates are noted; these typically refer to the number of children with dyslexia receiving services in public schools. Differences in prevalence rates based on testing every child in a class for a reading problem compared to data based on the number of children receiving special education services were exemplified by the findings of the Connecticut Longitudinal Study (CLS). The CLS, based on a population representative of all children attending public kindergarten in Connecticut, assessed reading and intelligence in each child in the study and found that one in five children was dyslexic. This figure contrasts sharply with data based solely on numbers of children receiving special educational services, which is much smaller, about 5%. Clearly, many struggling readers are not identified by their schools.
Dyslexia affects just about as many girls as boys. It is used to be thought that dyslexia affected primarily boys, and as a result, mainly boys were identified; girls who were sitting quietly at their desks – and not reading – tended to be overlooked. This reflects what is referred to as selection bias. For example, in the CLS, not only was each child individually tested, but the researchers also obtained data on which children were identified by their schools as having a specific reading disability. While comparable numbers of boys and girls were found to be dyslexic when each child was tested, four to five times as many boys compared to girls were identified by schools. Why? The data showed that teachers tended to refer for further evaluation boys who were more active and impulsive. In contrast, girls – who were not learning to read, but who were perceived as behaving more “properly” – were not identified by their schools as having a reading problem. It seems teachers often incorporate a “norm” for behavior for both boys and girls that is more typical of girls. As a result, boys who may be behaving on the higher end of normal rambunctious behavior for boys, are considered to be behaving poorly and referred for further evaluation.
Does dyslexia ever go away?
Dyslexia does not resolve over time. Longitudinal studies indicate that dyslexia is a persistent, chronic condition; it does not represent a transient “developmental lag.” The image below shows the trajectory of reading skills over time in good and poor readers. The vertical axis on the left is the reading achievement score from the Woodcock-Johnson reading test, and the horizontal axis is the age in years. Both good (upper curve) and poor readers (lower curve) improve their reading scores as they get older, but the gap between the dyslexic and the non-impaired readers remains.
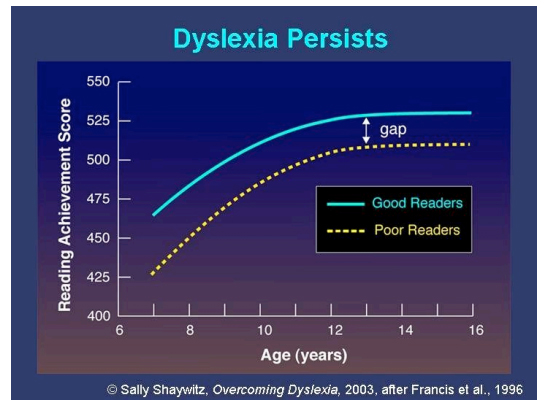
The proven persistence of dyslexia is a critical finding: children who present with reading difficulties early on must be helped immediately rather than waiting in the belief that the reading difficulties are temporary or that they will be outgrown. While dyslexia is not cured, it can be helped greatly by early and effective, scientifically-based reading interventions. (See below: Teaching Reading and Remediating Reading Difficulties)
The Cognitive Basis of Dyslexia
Why do otherwise bright, motivated children struggle to learn to read?
Dyslexia reflects a very specific difficulty with reading and has nothing to do with intelligence. In fact, understanding ideas and concepts are often at a very high level in dyslexia as are other higher-level reasoning skills. Dyslexia is a localized problem, one involving the sounds, and not the meaning, of spoken language. Consideration of the differences between spoken and written language provides a helpful understanding of why some bright children struggle to read.
First, let us consider spoken language. We, as humans, have beenspeaking for hundreds of thousands years; speaking is part of the human condition. Everyone learns to speak, speaking is natural; simply place a baby in a spoken language environment and that child will learn to speak. No need to develop a spoken language curriculum for babies.
Reading is different, it is a relatively recent invention of man and many societies still rely on speaking, rather than reading. In contrast to speaking, which is natural and spontaneous, reading is artificial and must be taught. The question is: what must be learned in order to transform the printed letters on the page to words that have meaning? Today, science has provided the answer: the letters must be connected to something that already has inherent meaning – the sounds of spoken language. And so, in order to learn to read, children must learn how to link the printed letters on the page to the sounds of spoken language. To do this, a child must first develop the awareness that spoken words can be pulled apart into their constituent parts; for example, that the word, mat is made up of three underlying sounds – “mmm,” “aaaa,” “t.” For about 60-70% of children, this awareness develops readily by the age of about six years. In contrast, another 30- 40% experience difficulty noticing these basic sounds, called phonemes that make up all spoken and written words.
Try it yourself, for example, can you say the word “steak” without the “t” sound? Answer: “sake.” To do this, you had to pull apart the Sounds- – “sss” “t” “aaa” “k” — that make up “steak” and pull out the “t” sound and then push the remaining sounds back together so that “sake” remains. These sounds, called phonemes (defined as the smallest unit of speech that distinguishes one word from another) are the basic building block of all spoken and written words. In English, there are forty-four phonemes. In speaking, a person utomatically goes to his/her internal dictionary and retrieves the appropriate phonemes that make up a word, orders them correctly, and then utters the word. For most people, the phonemes are clear and crisp, but for reasons yet unknown, in people with dyslexia, the phonemes are less clear; they are fuzzy and less distinct. And this has important implications for both speaking and reading. In speaking, people with dyslexia sometimes retrieve a phoneme that sounds similar to the one they intended; the result is that a dyslexic sometimes intends to say one word but ends up saying a word that sounds similar. For example, a child who is dyslexic was at a ballgame where she became thirsty and asked her mother to take her to the “confession” stand. Of course, she meant, “concession” stand but pulled out — not the exact sound — but one that was very similar to the sound she intended.
This difficulty in spoken language is common in dyslexia; its practical significance is that it provides a clue that a child may be at-risk for dyslexia, even before she is expected to read. Such word confusions are important clues for parents and teachers to be aware of, and to recognize that they are sound-based and not meaning-based mistakes. The person who is dyslexic knows the word s/he wants to say, but just has trouble pulling the correct sound out of his/her internal dictionary. Even in adults, such sound-based or phonological confusions (derived from the Greek word “phone” meaning sound) are often a clue that a person may be dyslexic.
In reading, the importance of being able to pull apart the sounds of spoken words and isolate individual sounds is that the individual sounds of spoken words represent the links, the Velcro, on which to connect the letters in words. If a child (or adult) cannot isolate the individual sounds, he does not have anything with which to link the letters in a word. And so, the fundamental steps in learning to read are:
• Developing the awareness that a spoken word can be pulled apart into smaller units or phonemes, technically, this is referredto as phonemic awareness. Keep in mind that this basic first step in learning to read involves spoken language.
• Linking each letter in a word to the individual sound it represents. This is referred to as phonics
Once children appreciate that the printed word has the same number and sequence of sounds as the spoken word, they have mastered the alphabetic principle and are ready to read. It is important to remember that all children, the very best readers, the poorest readers, and all those in-between, must take the very same steps to becoming a reader. The difference, of course, is in the time and effort that it takes.
In summary, in order to read, a child has to develop the insight that spoken words can be pulled apart into the elemental particles of speech (phonemes) and that the letters in a written word represent these sounds. Accumulating evidence indicates that this difficulty with the sounds of spoken language is largely missing in dyslexic children and presents a persisting difficulty in adults who are dyslexic. A quote that captures this relationship between spoken and written language comes from Bloomfield, who wrote, “Writing is not language, but merely a way of recording [spoken] language by visible marks.”
Making a Hidden Disability Visible
Imaging reading and dyslexia
Dyslexia is a hidden disability; people who have it are often bright and have no outward signs of a problem. If a person has a broken arm, it is visible to all. If a person is dyslexic, how can you look within his or her brain to see the root of the problem? For many, many years, this presented a significant problem for those who are dyslexic. Because their reading difficulty is by definition, unexpected, and they seemed to have all the cognitive equipment necessary to be good readers, dyslexic children were often undiagnosed, misdiagnosed, or worse, accused of not trying hard enough or of being not motivated or of being “stupid.” Since people who are dyslexic have no outward visible signs of their difficulty, many even questioned the very existence of dyslexia.
In the 21st century, with the advent of functional brain imaging, this has all changed. In our laboratory, one of the very first to image dyslexia, we have now imaged several thousand children and adults as they read or attempt to read. Functional magnetic resonance imaging (fMRI) is similar to MRI; if you have ever had an MRI for a headache or knee injury, fMRI and MRI use a similar scanner. fMRI, shown in the image above, uses somewhat more sophisticated hardware and software that allow it to capture brain changes (mainly blood flow) as a person performs a specific cognitive task, for example, reading.
Data using fMRI from laboratories around the world indicate three neural systems for reading shown in the image below. These are all located in the left side of the brain: one in the front of the brain (shown in green, in the region of the inferior frontal gyrus [Broca’s area]) and two in the back of the brain (one in the parieto-temporal region, shown in red, and a second in the occipito-temporal region, shown in yellow).
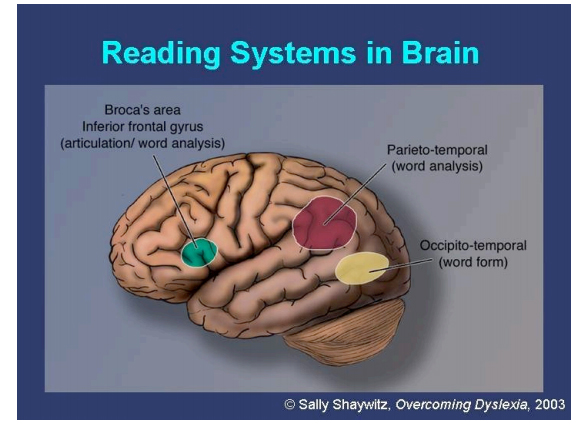 The latter system (found behind the ear in the area where children often have swollen glands) is of particular importance for skilled, fluent reading and is termed the visual word-form area (VWFA). Neural systems in dyslexia
The latter system (found behind the ear in the area where children often have swollen glands) is of particular importance for skilled, fluent reading and is termed the visual word-form area (VWFA). Neural systems in dyslexia
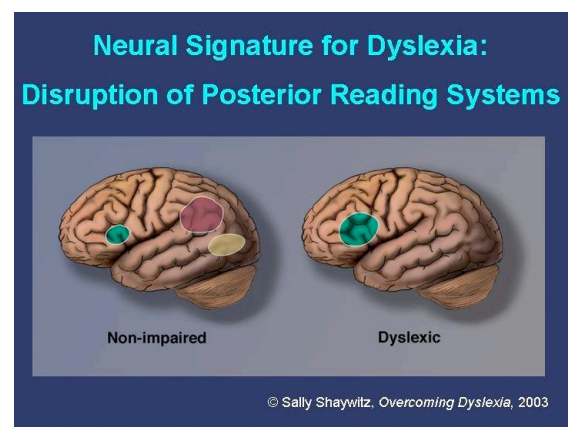
In dyslexic readers, converging evidence from many laboratories around the world has demonstrated “a neural signature for dyslexia,” that is, a disruption of the two neural systems in the back of the brain observed during reading (shown in the image below).
In nonimpaired readers, three systems are evident, one anterior in the area of the inferior frontal gyrus (shown in green) and two posterior, the top system around the parieto-temporal region (shown in red) and the bottom system around the occipito-temporal region (shown in yellow).
In dyslexic readers, the anterior system is slightly overactivated compared to non-impaired readers; in contrast, the two posterior systems are underactivated. This pattern of underactivation in left posterior reading systems is referred to as the neural signature for dyslexia. Brain imaging now provides visible evidence of the reality of dyslexia; dyslexia is no longer a hidden disability.
Imaging also reveals compensatory overactivation in other parts of the reading system. The compensatory neural systems allow a dyslexic person to read more accurately. However, the critical visual word-form area remains disrupted and difficulties with rapid, fluent, automatic reading persist. The dyslexic continues to read slowly.
Neurobiological evidence is beginning to emerge indicating that many dyslexics are not able to make good use of sound-symbol linkages as they mature, and instead, they come to rely on memorized words. A recent fMRI study also demonstrates the importance of memory systems in dyslexic readers. Together, these recent neurobiological findings suggest that as dyslexic children mature, neural systems supporting word memorization develop, rather than the systems supporting sound-symbol linkages and automatic reading that are observed in typical readers.
Functional imaging has been helpful in demonstrating that the neural systems for reading are malleable, and that the disruption in these systems in young struggling readers can be modified by an effective reading intervention (see below: Teaching Reading and Remediating Reading Difficulties). Compared to struggling readers who received other types of intervention, children who received an experimental intervention (which focused on evidence-based application of the alphabetic principle) not only improved their reading but, compared to pre-intervention brain imaging, demonstrated increased activation in the neural systems for reading. These data have important implications for public policy regarding teaching children to read: the provision of an evidence-based reading intervention at an early age improves reading and facilitates the development of those neural systems necessary for reading.
Translating Research into Practice
Clues to a Diagnosis of Dyslexia
Dyslexia is more than simply a score on a reading test. Reflecting the core sound-based phonological deficit, a range of downstream effects is observed in spoken as well as in written language. Phonological processing is critical to both spoken and written language. While most attention has centered on the print difficulties, spoken language is also affected. The ability to notice, manipulate, and retrieve individual sounds (phonemes) has an important function in speaking, for example, a person must retrieve phonemes from his/her internal dictionary lexicon and serial order them correctly in order to utter the spoken word. Thus, it should not be surprising that problems with spoken language, albeit more subtle than those in reading, are often observed.
Clues to spoken language difficulties in dyslexia: (source © Overcoming Dyslexia, S.Shaywitz, Knopf, 2003, pp.122- 123;
http://www.amazon.com/Overcoming-Dyslexia-Complete-Science-Based-Problems/dp/0679781595)
• late speaking
• mispronunciations
• difficulties with word retrieval
• needing time to summon an oral response
• confusing words that sound alike, for example, saying “recession” when the individual meant to say, “reception”
• pausing or hesitating often when speaking
• using lots of “um’s” during speaking, lack of glibness
• using imprecise language, for example, “stuff,” “things,” instead of the proper name of an object
• underestimation of knowledge, if based solely on (glibness) of oral response
As reflected in the spoken language difficulties in dyslexia noted above, it is apparent that dyslexics are not glib, particularly when put on the spot for a quick response. Keep in mind: this is not a matter of knowing the answer. Rather, the problem – when the person knows the answer – is in pulling the word out and saying it, that is, in retrieving the spoken word instantly. Glibness should not be taken as a measure of understanding, especially in a person who is dyslexic.
A range of difficulties is noted in reading at all ages. Awareness of these signs is important and may lead to earlier and more accurate diagnosis of dyslexia in children and adults. Specific clues to dyslexia noted in reading are listed below.
Clues to Reading Difficulties in Dyslexia: (source © Overcoming Dyslexia, S.Shaywitz, Knopf, 2003, pp.123- 124;
http://www.amazon.com/Overcoming-Dyslexia-Complete-Science-Based-Problems/dp/0679781595)
• Slow progress in acquiring reading skills
• Lack a strategy to read new, unknown words – trouble sounding out unfamiliar words
• Inability to read small, so-called function words such as “that,” “an,” “in”
• Terrific fear of reading aloud; avoidance of oral reading
• Oral reading filled with mispronunciations, omissions, substitutions
• Oral reading that is choppy and sounds like reading a foreign language
• Reliance on context to discern the meaning of what is read
• Disproportionate poor performance on multiple choice tests
• Slow reading
• Reading is tiring
• Inability to finish tests on time – doesn’t finish or rushes and makes careless errors; final test grade does not reflect person’s knowledge of the topic
• Disastrous spelling
• Homework that never seems to end; parents recruited as reader
• Messy handwriting despite what may be an excellent facility at word processing
• Extreme difficulty learning a foreign language
• Avoidance of reading for pleasure which seems too exhausting
• Reading effortful, demands extra attention and concentration to read
• Requires quiet environment to concentrate on reading
• Reading accuracy improves over time, though it continues to lack fluency and remains laborious and slow
• Lowered self-esteem with pain that is not always visible to others
• Development of anxiety, especially in test-taking situations
• History of problems in reading, spelling, foreign language learning in family members
The lack of reading fluency brings with it a need to read “manually” (a process consuming great effort and time), rather than automatically; the cost of such reading, in addition to reading slowly, is a tremendous drain on attentional resources. This is often observed in the classroom when struggling readers are asked to read quietly, deplete their attentional resources as they struggle with the print, and, as a consequence, appear to be daydreaming or not attending to the assigned reading. An additional cost to the person is that non-fluent or “manual” reading is very tiring to the person.
Sea of Strengths Model of Dyslexia
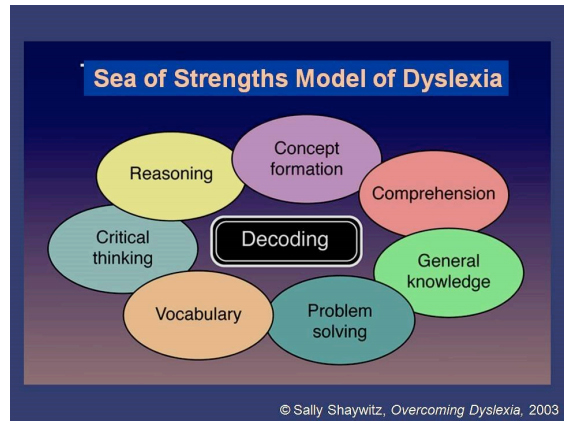 In contrast to the spoken language and reading difficulties in dyslexia, other abilities, particularly higher level cognitive abilities including thinking, reasoning, vocabulary, and problem solving are usually intact. This conceptual model of dyslexia has been referred to as a Sea of Strengths Model of Dyslexia (shown in image above). This model considers dyslexia to be an encapsulated or circumscribed weakness in decoding surrounded by a range of higher level cognitive strength. In diagnosing dyslexia, the goal is to identify both the strengths and the weakness and in managing dyslexia, the weakness is remediated and the strengths are acknowledged and facilitated. A critical component of managing dyslexia, as discussed below, is to ensure that people who are dyslexic are able to access their strengths and this is most commonly achieved through the provision of accommodations such as extra time on examinations.
In contrast to the spoken language and reading difficulties in dyslexia, other abilities, particularly higher level cognitive abilities including thinking, reasoning, vocabulary, and problem solving are usually intact. This conceptual model of dyslexia has been referred to as a Sea of Strengths Model of Dyslexia (shown in image above). This model considers dyslexia to be an encapsulated or circumscribed weakness in decoding surrounded by a range of higher level cognitive strength. In diagnosing dyslexia, the goal is to identify both the strengths and the weakness and in managing dyslexia, the weakness is remediated and the strengths are acknowledged and facilitated. A critical component of managing dyslexia, as discussed below, is to ensure that people who are dyslexic are able to access their strengths and this is most commonly achieved through the provision of accommodations such as extra time on examinations.
How dyslexics think
As noted above, dyslexia is more than a score on a reading test. In fact, dyslexia is more than just a reading difficulty, it is a way of thinking and of being. Differences in brain organization not only give rise to slow reading, they also generate a different way of thinking. Intact higher level abilities offer an explanation of why reading comprehension is often appreciably above single word reading accuracy and fluency in dyslexia. Often strong vocabularies and strong conceptual skills enable a dyslexic to figure out a word or the gist of a paragraph even when that person cannot decipher the specific word on the page.
Dyslexics tend to be top-down rather than bottom-up thinkers; that is, they learn from getting the big picture or the overall idea or leaning first, and then fill in the specific details. People who are dyslexic learn best through meaning, by understanding the overall concept or main idea rather than through rote memorization of isolated facts.
Strong visualization skills are also an asset to those who are dyslexic.
Making a diagnosis of dyslexia
Dyslexia is a clinical diagnosis, best made by an experienced clinician who knows the individual, has taken a careful history, observed the child or young adult reading, and administered a battery of tests that assess the child’s intelligence, academic skills including reading accuracy, fluency and comprehension, spelling, mathematics (which is often high), and language skills, particularly phonological processing (getting to the sounds of spoken language). The uneven peaks and valleys of cognitive and academic functioning both contribute to the clinical picture of dyslexia: a weakness in phonologically-based skills in the context of stronger cognitive and academic skills in non-reading related areas.
The critical element is the unexpected nature of the reading difficulty, that is, it is unexpected in relation to a person’s age, intelligence, education, and professional status. And so, if a person has an IQ in the superior range or is a physician or an engineer and has a reading accuracy score in the so-called “average” range, there is a disparity between that individual’s ability, education or training, and his/her reading achievement – that person is dyslexic. Just recently, in our laboratory, using longitudinal data from the CLS, our research team has been able to demonstrate that in good readers, intelligence and reading are linked and mutually influence one another over time.
However, and critically, in the case of dyslexia, intelligence and reading go their separate ways, are not linked, and do not influence one another. This finding provides important empirical evidence to support the definition of dyslexia as an unexpected difficulty in reading.
This dissociation in dyslexia between intelligence and reading also provides strong evidence for the findings of low reading achievement in the presence of strong intellectual abilities in people who are dyslexia.
As children mature compensation often occurs, resulting in relatively accurate, but not fluent, reading. Awareness of this developmental pattern is critically important for the diagnosis in older children, young adults, and beyond. The consequence is that such dyslexic older children may appear to perform reasonably well on a test of word reading or decoding accuracy; on these tests credit is given irrespective of how long it takes for the individual to respond or if there are initial errors in reading that are then corrected. Accordingly, tests of reading fluency – how quickly and accurately — individual words and passages are read aloud and tests assessing reading rate are keystones of an assessment for, and an accurate diagnosis of, dyslexia.
What do you do if you suspect a reading problem in your child?
Do not wait!! We now know that reading difficulties are persistent. Teachers and parents, too, often rationalize: it’s just a developmental lag; she’ll outgrow it; he’s a boy. Early on, in preschool or kindergarten, a child – who has difficulty learning the names of the letters and then the sounds associated with each letter or letter group, and doesn’t seem to be able to learn how to sound out words – should be considered at-risk and assessed for a possible reading problem. At this early stage, often a speech and language pathologist is extremely helpful in assessing the spoken language skills that represent the foundation for learning to read. As a child matures and seems to be struggling with reading and exhibiting the difficulties in spoken and/or written language noted above, that child should receive a full evaluation for the possibility of dyslexia. Children learn about three thousand new words a year; in the US, children tend to be identified as dyslexic in third grade or often, much later. This means that these struggling readers are already behind in learning ten thousand or so words; a terrible burden to place on a child – especially when there are highly effective reading interventions now available.
Other considerations in making a diagnosis of dyslexia:
As in other important medical conditions, the history is critical and should be given prominence in the diagnostic formulation. Observing the person read and administering tests are ancillary and helpful. Since vision and hearing are critical for reading, children and adults who are experiencing difficulty in reading should have their hearing and vision checked. There are no laboratory tests other than cognitive, language, and reading that are necessary to make a diagnosis of dyslexia. While brain imaging is a very helpful research tool, it is not yet reliable enough when used on individuals (rather than with groups) to be used as a diagnostic tool. Similarly, while there is research exploring possible genetic links to dyslexia, this is still in its early stages and there are currently no reliable genetic tests for dyslexia. Most likely, there are several genes governing the reading process and much more work to be done. An additional consideration in making the diagnosis is the role of attention. Attention is critical for learning to read as part of the reading process itself. Struggling readers require large amounts of attention, sometimes more than they can provide. In addition, there is a significant overlap or high “co-morbidity” between the occurrence of dyslexia and attention-deficit/hyperactivity disorder (ADHD). Both frequently occur in the same individual. Consequently, a consideration of the possibility of an accompanying ADHD should also be considered in those diagnosed with dyslexia; similarly, dyslexia should be considered as a possible additional diagnosis in those diagnosed as ADHD.
Essentials of Dyslexia Management:
I. Teaching Reading and Remediating Reading Difficulties
All children must take the same steps in learning to read. Accordingly, the basic components of reading that must be mastered are shared by all readers: good readers and struggling ones. What and how to most effectively teach reading now has a scientific basis. In 1998, Congress, concerned about what seemed to be a growing epidemic of reading difficulties in children, mandated that a National Reading Panel (NRP) be appointed to carefully review and assess the scientific data on teaching children to read. One of us (SS) was honored to serve on the NRP and in April, 2000, presented the Report of the NRP to the US Congress. Basically, the Panel found that the most effective, evidence- based approach to teaching reading must include five critical components:
1. Phonemic awareness: the ability to be aware of, notice, or manipulate the sounds of spoken language
2. Phonics: learning to link letters to the sounds they represent
3. Fluency: the ability to read both accurately and rapidly, and with good intonation
4. Vocabulary: to understand the meaning of words read
5. Comprehension: to understand and discern the meaning of connected text
Furthermore, these components are most effectively taught in an explicit, systematic approach. For struggling readers, it is critical that, in addition to an evidence-based approach:
• Instruction is intense, that is, in small groups not greater than 4-5 students;
• Sufficient time is devoted to teaching reading and language-related skills, for example, sixty to ninety minutes, optimally, each day;
• Support services are provided to children until they become not only accurate, but also fluent for most words at their grade level;
• Accommodations are provided to permit dyslexic students to demonstrate their knowledge
Just as for other important conditions that affect the health and welfare of children where we expect physicians to prescribe the most effective, proven treatments, today, in education, science has progressed so that it is now possible, and indeed, mandatory, that children be taught reading by evidence-based, proven methods. Such evidence-based approaches have been found to be highly effective for improving reading in children who are dyslexic. Interventions focused at word decoding and single word identification levels have had the most consistent evidence and have been shown to be the most effective, particularly in prevention and early childhood studies. Fluency and comprehension focused interventions have had less investigation, but have still shown some, albeit more variable, effects on reading outcomes in these students. Programs that systematically integrate multiple-focused interventions are considered to be the most effective, although their specific sequencing, degree of overlap, and level of focus on each component during each phase are still open to critical investigation. There is no single program that is head and shoulders above other evidence-based programs. Up-dates on the most recent evidence evaluating the efficacy of reading programs are found on the What Works Clearing House Web site (www.whatworks.ed.gov) of the Institute for Educational Sciences of the US Department of Education.
II. Providing Accommodations
Accommodations that Help Level the Playing Field
A complete education for a dyslexic student includes evidence-based reading interventions and accommodations. As noted above, intervention data, while promising, have yet to indicate closing the gap in the ability to read words fluently in children beyond the first few grades. Accordingly, although dyslexic children will improve their accuracy, lack of fluency (slow, effortful reading) continues to be a concern at all grade levels, increasingly so as children move up into middle and high school and then into postsecondary education.
Accommodations are of three general types:
1) Those that by-pass the reading difficulty by providing information through an auditory mode;
2) Those that provide compensatory assistive technologies; and,
3) Those that provide additional time so that the dysfluent reader can demonstrate his/her knowledge.
First, beginning quite early in their schooling, dyslexic readers require alternative modes of acquiring information so that their vocabulary and fund of knowledge more closely reflect their intellectual level than their impaired reading ability. Access to recorded materials, for example, from Recordings for the Blind & Dyslexic (www.rfbd.org), whether they are based on the school curriculum or reflect what peers are reading for pleasure, are a necessity for such children if they are to keep up with their classmates and with their own intellectual curiosity and interests. Next, assistive technology, computers with both print-to- speech as well as speech-to-print software, provide further compensation for oft-noted difficulties with handwriting, spelling, and lack of fluency.
The Scientific Basis for the Necessity for Accommodations for Dyslexia
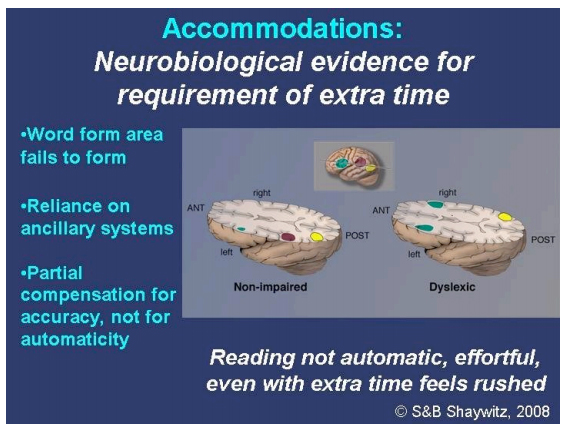
A major advance has been the convergence of behavioral and neuro-imaging data providing evidence for the critical need for extra-time on examinations for dyslexic students, particularly as they progress towards high school graduation and beyond. Thus, ehavioral data indicating the persistence of dysfluent reading are now supported by neurobiological data. The image above shows cut-away views of the brain in non-impaired readers (left) and dyslexic readers (right). As noted earlier when describing the neural signature of dyslexia, in dyslexic readers the posterior reading systems, especially the left occipto-temporal (word-form) region responsible for fluent, rapid reading, is disrupted in dyslexic children and adults. Other compensatory systems, in the frontal regions on both left and right hemispheres (shown in green), and the right hemisphere homologue of the word form area develop, and these systems support increased accuracy over time. However, the word-form region does not develop and compensatory pathways do not provide fluent or automatic reading. Accordingly, if such students are to demonstrate the full range of their knowledge, providing additional time on examinations is a necessity to compensate for the lack of availability of the efficient word-form area and to level the playing field.
How much extra time is best determined by the student’s own experience of trial and error over the years. Currently, there are no quantitative data available to serve as a reliable metric for gauging the specific amount of time needed by a student. Since longitudinal data, both behavioral and imaging, indicate persistence of the reading difficulty, requiring that students in postsecondary settings be tested every three or five years is not consistent with scientific knowledge. Furthermore, it is extremely expensive and even problematic.
As students progress through school to higher grades, and compensate in reading accuracy, simple reading measures of word identification fail to capture difficulties in fluent reading and so are often misleading. In addition, since such non-automatic readers must call upon attentional resources during reading, they are highly susceptible to noise and distractions. Study and test-taking in quiet, separate rooms allow these dysfluent readers to concentrate and make maximum use of their often strained attentional resources.
People who are dyslexic are entitled to protection from discrimination under the Americans with Disabilities Act (ADA). Here are some helpful things to know about accommodations:
• In making assessments of an individual who is dyslexic for purposes of providing accommodations under the ADA, that person’s reading must be compared with others of comparable education, intelligence, and professional status.
• Studies have shown that providing accommodations provides no special advantage to dyslexic individuals, it just levels the playing field. It is important to know that non-dyslexic readers do not show a significant increase in test scores with extra time, while people who are dyslexic show a highly significant increase in scores. (Image 6; link to ADA Congressional testimony).
• A Blue Ribbon Panel convened to determine the necessity for “flagging” tests taken with accommodations determined that such flagging was not appropriate. (See link to www.dra.org for full report of the Panel).
• Dyslexia is life-long; there is no necessity and it is, in fact, inappropriate to require repeated testing after a person is diagnosed as dyslexic.
In summary, given that dyslexia represents a disparity between an individual’s reading and intellectual abilities; accommodations are critical to assure fairness and equity. Contemporary management of dyslexia provides evidence-based accommodations; these include: access to recorded materials; computers and print-to-speech software; additional time on examinations, with amount of time determined by the student’s experience. Tests are often inadequate proxies; the reality of life experience in dyslexia provides the most valid evidence for a person’s need for accommodations. In addition, it is inappropriate to assess a dyslexic person’s knowledge based on his/her performance on an oral examination in which that individual is under pressure to provide a quick or glib response.
Accommodations are provided based on a student’s history, observations of his/her reading aloud, and test results; once a student is diagnosed as dyslexic, the evidence indicates this is a persistent, life-long difficulty. With provision of such accommodations, dyslexic students are entering and succeeding in a range of professions including journalism, literary writing, science, medicine, law, and education.
Adult Outcome of Dyslexia
Over time, reading accuracy improves so that dyslexic readers are able to read, albeit slowly and with great effort. In contrast, dyslexic readers continue to lack fluency. The basic phonologic difficulty persists; spoken language difficulties remain.
Problems in speaking in adult dyslexics: (source ©S. Shaywitz, Overcoming Dyslexia, Knopf, 2003, pp.125- 126;
http://www.amazon.com/Overcoming-Dyslexia-Complete-Science-Based-Problems/dp/0679781595)
• Mispronunciation of names of people and places
• Difficulty remembering names of people and places
• Confusion of names that sounds alike
• Struggle to retrieve words, “It was on the tip of my tongue”
• Lack of glibness, especially if put on the spot
• Spoken vocabulary smaller than listening vocabulary
• Hesitation to say aloud words that may be mispronounced
Problems in reading in adult dyslexics: (source ©S. Shaywitz, Overcoming Dyslexia, Knopf, 2003, pp.125- 126; http://www.amazon.com/Overcoming-Dyslexia-Complete-Science-Based-Problems/dp/0679781595)
• Childhood history of reading and spelling difficulties
• Word reading more accurate, but still effortful
• Lack of fluency
• Embarrassment caused by oral reading: avoidance of Bible study group, reading at Passover seders, or delivering a written speech
• Trouble reading and mispronouncing uncommon or strange words such as people’s names, names of streets or locations, food dishes on the menu • Substitution of made-up words, during reading, for words that cannot be pronounced, for example, metropolitan becomes mitan
• Extreme fatigue from reading
• Slow reading of most material: books, manuals, subtitles to foreign films
• Penalized by multiple choice tests
• Unusually long hours spent reading school or work materials
• Frequent sacrifice of social life for studying
• Preference for books with figures, charts, or graphics
• Preference for books with fewer words per page or with lots of white showing on the page
• Disinclination to read for pleasure
• Spelling remains disastrous; in written work, preference for less complicated words that are easier to spell
• Particularly poor performance on rote, clerical tasks Strengths in higher level thinking processes
• High learning capability
• Noticeable improvement when given additional time on multiple choice tests
• Noticeable excellence when focused on a highly specialized area such as medicine, law, public policy, finance, architecture, basic science
• Excellence at writing if content and not spelling is important
• Noticeable articulateness in expression of ideas and feelings
• Exceptional empathy and warmth and feeling for others
• Success in areas not dependent on rote memory
• Talent for high level conceptualization
• Ability to come up with original insights
• Big picture thinkers
• Inclination to think out-of-the-box
• Noticeable resilience and ability to adapt
Reflecting these strengths, dyslexics are often high level conceptualizers who manifest “out-of-the-box thinking” and are frequently the ones who provide new insights. As a person who is dyslexic progresses and is able to specialize in an area, s/he may become relatively automatic in reading the vocabulary recurring in that area. Dyslexics are often represented at the higher levels of a range of professions and are frequently found as leaders in such diverse areas as science, medicine, law, business, writing/literature, poetry.
Dyslexic writers and playwrights:
John Irving
Stephen J. Cannell
Wendy Wasserstein
Dyslexic financiers or entrepreneurs:
Charles Schwab,
Sir Richard Branson,
John Chambers (Cisco Systems),
William Hewlett,
Paul Orfalea (Kinko’s),
Ingvar Kamrad (IKEA),
Ted Turner
As Charles Schwab recalls,
“Even though I couldn’t read quickly, I could imagine things much faster than some other people who were stuck thinking sequentially. That helped me in solving complex business problems. I could visualize how things would look at the end of the tunnel.”
© Overcoming Dyslexia, S. Shaywitz, 2003, p. 357.
Dyslexic scientists:
Nobel laureates: Albert Einstein, Nils Bohr, Barry Benacerraf;
Dyslexic physicians:
Harvey Cushing – father of neurosurgery
Dr. Helen Taussig – helped develop Blalock-Taussig operation for “blue babies;”
Dr. Jack Barchas – leading psychiatrist
Dr. Delos Cosgrove – led the Department of Cardio-Thoracic Surgery at the Cleveland Clinic to International prominence and has at least 20 patents for advances in valvular surgery. Dr. Cosgrove is now CEO of the Cleveland Clinic.
Looking to the Future
There is now evidence of both the weakness and the strengths associated with dyslexia. The weaknesses have been well elaborated and described; the strengths are often overlooked. To illuminate and focus attention on the strengths associated with dyslexia and to inform society about the newest knowledge of dyslexia, the Yale Center for Dyslexia and Creativity (with the tag-line: slow reader, out-of-the-box thinker) has now been established at Yale University (Website: www.dyslexia.yale.edu). The mission of the Center is to use the power and authority of modern science to transform dyslexia from a liability to a strength, so that his or her strengths rather than weaknesses come to define a dyslexic person’s life. The Center is actively involved in large scale dissemination and education initiatives – to produce a paradigm shift and advance societal attitudes about dyslexia. These efforts are targeting K- 12 as well as higher education, medicine, business, law, policy, the media, and other innovative, scholarly initiatives to better identify dyslexia and to define the link between dyslexia and creativity.
Websites:
http://www.amazon.com/Overcoming-Dyslexia-Complete-Science-
Based-Problems/dp/0679781595
www.dyslexia.yale.edu
www.professorgarfield.org
www.sparktop.org
www.whatworks.ed.gov
www.dralegal.org
www.rfbd.org
www.audible.com
www.bookshare.org
www.asha.org
Books about Dyslexia
Shaywitz, S. (2003). Overcoming Dyslexia: A new and complete science-based program for reading problems at any level. New York, NY: Alfred A. Knopf.
Report of the National Reading Panel. (2000). Teaching Children to Read: An Evidence Based Assessment of the Scientific Research Literature on Reading and its Implications for Reading Instruction (Vol. NIH Pub. No. 00-4754): U.S. Department of Health and Human Services, Public Health Service, National Institutes of Health, National Institute of Child Health and Human Development.
References
1. Shaywitz, S., Morris, R., & Shaywitz, B. (2008). The education of dyslexic children from childhood to young adulthood. Annual Review of Psychology, 59, 451-475.
2. Shaywitz, S. E. (1996). Dyslexia. Scientific American, 275(5), 98- 104.
3. Shaywitz S, Shaywitz B. Dyslexia (specific reading disability). Biol Psychiatry 2005;57: 1301–9.
4. Dehaene, S., Cohen, L., Sigman, M., & Vinckier, F. (2005). The neural code for written words: a proposal. Trends in cognitive sciences, 9(7), 335-341.
5. Shaywitz, B., Skudlarski, P., Holahan, J., Marchione, K., Constable, R., Fulbright, R., et al. (2007). Age-related changes in reading systems of dyslexic children. Annals of Neurology, 61, 363-370.
6. Paulesu E, Demonet J-F, Fazio F, McCrory E, Chanoine V, et al. 2001. Dyslexia-cultural diversity and biological unity. Science 291:2165–67
7. Marzola E, Shepherd M. 2005. Assessment of Reading Difficulties. In Multisensory Teaching of Basic Language Skills, J.R. Birsh, Editor, Paul H Brookes, Baltimore, MD: pp. 171- 185.
8. Reynolds, C.R. (2008). RTI, Neuroscience, and Sense: Chaos in the Diagnosis and Treatment of Learning Disabilities, in Neuropsychological Perspectives on Learning Disabilities in the Era of RTI: Recommendations for Diagnosis and Intervention, E. Fletcher-Janzen and C.R. Reynolds (Eds.), John Wiley & Sons, Hoboken, NJ.